A Closer Look at Medical Adhesive Tapes for Diagnostic Applications
Adhesives and tapes used for diagnostics are faced with different challenges than those for skin contact and other medical applications.
When someone mentions medical adhesives, the first thought that often comes to mind is skin adhesion. It’s understandable, since nearly everyone has worn some type of medical adhesive product—from a simple bandage to an electrode, athletic tape, IV cover, and so on. However, an entire world of medical adhesives goes unnoticed by many: diagnostics.
What exactly do we mean by medical diagnostic adhesives? Specifically, we are referring to adhesive tapes used in the construction or assembly of in-vitro diagnostic devices. These devices are used either by consumers at home or by medical professionals to perform a series of tests (assays) to help achieve a diagnosis.
One of the most commonly known diagnostic devices is the at-home pregnancy test. The user places the sampling end of the device in the urine stream, waits a few minutes, and obtains a result (diagnosis). Another common and widely used example is a blood glucose test, or diabetic test strips. Approximately 17 billion test strips were used in North America in 2020, with an average price per strip at the pharmacy of $1.50. Revenues from blood glucose testing strips alone are greater than several skin adhesive markets combined.
In addition to home applications, endless diagnostic applications take place behind the scenes in labs and other medical facilities. For example, COVID-19 tests and blood samples from patient blood draws are taken to labs and placed onto devices where a series of assays occur. Through the analyzation of blood, saliva, urine, or tissue, hundreds of tests can be performed to provide insights into bodily functions or the presence of disease. Diagnoses can range from drug screening to cancer detection.
While different types of diagnostic devices vary in size, functionality, and complexity, nearly all utilize adhesives in some manner. Examples include:
- Urinalysis strips
- Lateral flow devices (e.g., pregnancy tests)
- Micro-fluidic devices (e.g., blood glucose, blood testing)
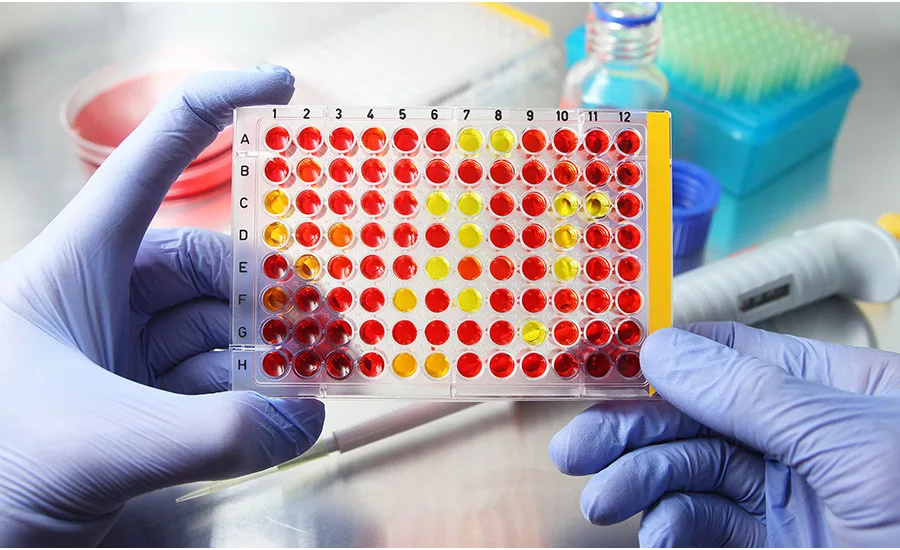
- Micro-titer plates (drug discovery and lab work)
- Microwells (microbial and pathogen detection)
- Microarray (genetic analysis)
- Polymerase chain reaction (PCR, DNA amplification)

In blood glucose testing, a small droplet of blood is taken from the finger and placed onto disposable, single-use testing strips for analysis.
Adhesive Requirements
Although each type of diagnostic device is unique in its workings, these devices share many similarities when it comes to adhesive requirements. One of the first questions asked of medical diagnostic adhesives experts is, “What regulatory requirements are associated with diagnostic adhesives?” Unlike skin adhesives, which must have ISO:10993 or USP Class VI to even be considered, no standardized testing requirements must be met for diagnostics. Patient safety isn’t a concern for the adhesive since it’s not going to be used on a patient. However, although it’s extremely rare, an adhesive approved for skin contact can also be suitable for use in diagnostic devices.
Skin adhesives rarely have the necessary level of cleanliness required for use in diagnostic applications. Skin adhesive applications have a much wider breadth of materials that are suitable for skin contact. The primary function of the skin is to act as a protective barrier against the harsh external environment and protect the delicate chemistries and biological process occurring inside the body. With in-vitro diagnostics, however, those chemistries and biological workings are taken from inside the protective environment of the body and placed into a much less favorable environment of a diagnostic device.
While the requirements for diagnostic adhesives depend on application, many similarities are shared among device types. Importantly, the adhesive must not interfere with any of the delicate chemistries or biological processes occurring within the device. Because of this requirement, diagnostic adhesives are the cleanest adhesives used in tapes.
These adhesives have extremely low outgassing, volatile organic compounds (VOCs), and adhesive component migration. The sensitive assay chemistries are easily corrupted by even the slightest impurity that could be imparted from the adhesive. In many instances, the volatile and migratory components of adhesives comprise sites of chemical functionality or reactivity. It is important that diagnostic adhesives be as inert as possible, with little to no residue chemical reactivity. Any residue monomer, crosslinker, vinyl functionality, reactive sites, or acid functionality can hinder or interfere with the device.
This is one of the main reasons water-based acrylic or rubber-based adhesives are not used in this market. With all the surfactants, wetting and defoaming agents, anti-microbial compounds, and more, water-based adhesives simply cannot meet even the least stringent of cleanliness requirements for diagnostic devices. Rubber-based adhesives are suitable in a few applications, but the large degree of unsaturation and antioxidant often interfere with various types of detection methods utilized.
In contrast, the pressure-sensitive adhesives (PSAs) that are used by tape manufacturers for diagnostic devices are pure acrylics or silicone adhesives with no additives or modifiers. These adhesives can be cast from solvent or coated using more modern ultraviolet (UV) curing techniques. It is necessary to apply extra drying and reaction/curing for these adhesives to ensure the cleanest, most inert adhesive possible.
Some types of assays rely on a form of optical detection or analysis involving light. These devices are commonly referred to as autofluorescence. Light at a particular wavelength is shined onto the device and excites the target analyte, which in turn emits (fluoresces) light back at another wavelength. The machine then measures to provide the result. Envision the effect of a black light shining on a white fabric or neon paint or ink. Adhesive tapes for these types of devices must be optically clear to the naked eye and to the wavelengths of light being used in order to excite and fluoresce back.
For comparison, the highest-end, ultra-clear polyethylene terephthalate (PET) adhesive laminates used in high-tech optical applications such as TV screens wouldn’t be suitable in these devices due to the way the adhesives absorb light, which would obscure the results. In addition to being clean, adhesives for diagnostic applications must be of specific monomer composition so as to not interfere with the transmission of light wavelengths.
The sample is excited with low-wavelength light during a fluorescence assay, while the target analyte emits higher wavelength red light that is measured and quantified
Diagnostic adhesives can be exposed to different environmental conditions, including prolonged exposure to acids, bases, alcohols, and many kinds of reagents and buffer solutions. Certain methods require the device be exposed to elevated temperatures (either continuously or cycled). It is essential that the adhesive maintain its chemical stability and adhesion integrity. In many devices, the adhesive is used to seal wells or channels containing fluids. If the adhesive bond begins to fail, this can lead to leakages and/or cross contamination that compromises the device’s functionality.
While it is necessary for the adhesive to aggressively bond to the many different types of plastics used in devices to prevent leakage, it’s also important that the adhesive doesn’t have too much flow. Many times, these properties work in opposition to each other. Devices, such as those that are microfluidic, work by transporting small amounts of biological fluids through very small channels through the device to reagents sites. The flow of fluids often relies on capillary action alone. If an adhesive has excessive creep, it’s very easy for the microchannels to become occluded, restricting capillary flow and ultimately leading to device failure. This can be exaggerated at elevated temperatures.

Microfluidic devices work by moving small amounts of a liquid sample from the collection site to a reaction site, which contains the assay reagents.
Difference in Adhesion
Although diagnostic adhesives must meet rigorous requirements in terms of cleanliness and inertness, adhesion and bonding requirements for these tapes are much simpler than those that are used to adhere to skin. Skin is by the far the most difficult and frustrating surface to design an adhesive tape for. Skin is not a static material but a complex, living, and fluid system comprising many different parts (see Figure 1). It’s constantly passing moisture, excreting oils, and regenerating/shedding itself.
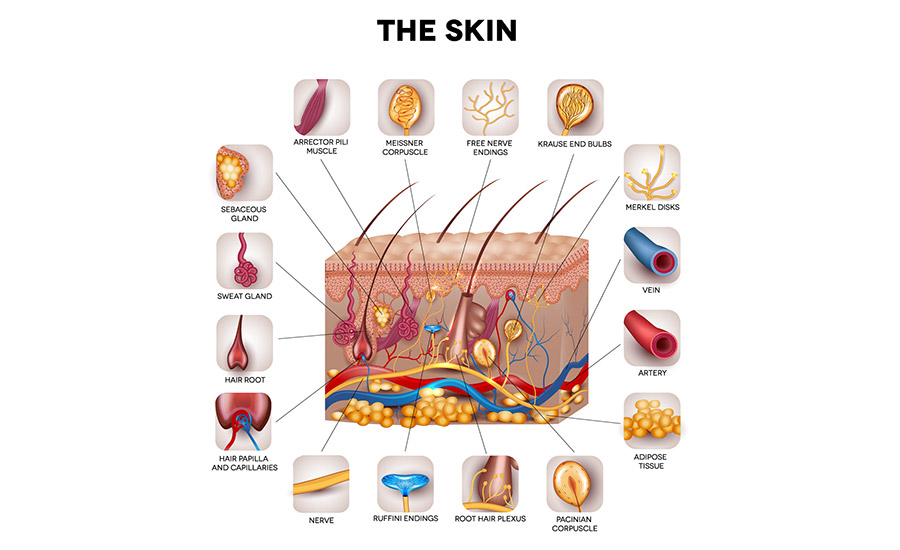
Figure 1. Skin is a complex, living, and fluid system comprising many different parts.
Skin is also responsible for the emotional responsiveness of the human sense of touch—put simply, it’s the primary source of pain response. Skin adhesion is the only application for adhesive products in which pain must be considered during product development.
The problem is that pain is subjective and hard to quantify. Every person has a different threshold for pain and discomfort. Pain responses from the same patient can even vary based on the area of the body. The rib cage and face area are more sensitive than the arms, for example. In addition, seasonality can influence how a patient reacts to an adhesive tape, as pain response is greater during the cold, dry winter months. With device manufacturers seeking to extend device wear times, balancing the moisture vapor transmission rates, aggressiveness, and pain/trauma upon removal becomes increasing difficult.
Another challenge product developers face with skin adhesion is generating tangible results. Even with the tight design window for cleanliness for diagnostic adhesives, it’s relatively easy to measure adhesive performance accurately, repeatedly, and with great accuracy. Analytical techniques such as headspace gas chromatography (GC) and Fourier-transform infrared spectroscopy (FTIR) analysis can be used to precisely measure performance, and test devices can always be made and evaluated for functionality.
Adhesion testing for diagnostic tapes is also easily performed. Samples can simply be placed in a testing instrument, and peel force is accurately and reproducibly reported. While the plastics used by suppliers may vary, adhesion to materials such as high-impact polystyrene, ABS, PE, PP, and TPO is relativity straightforward and well understood.
On the other hand, skin is much more difficult to test. We don’t have adequate predictive materials for skin adhesion. Even cadaver skin does not work well for lab evaluation purposes because it differs too much when compared to living skin. Unlike adhesion testing on rigid inanimate objects, it’s not practical to test peel adhesion off of skin using tape testers.
When designing adhesive tape products, scientists rely on practical testing and subjective user feedback, which must then be performed across a large data population. These evaluations frequently need to be repeated multiple times to ensure reproducibility and validate results. This can take months or even years, in some cases, and at significant expense.
For more information, visit www.mactac.com.
Note: Images courtesy of Mactac.
Looking for a reprint of this article?
From high-res PDFs to custom plaques, order your copy today!


